Question 9 of 16
(demo test)
Product Demo for CORE & APPLIED Exams
-
A 48-year-old male is ~3 months status-post Mohs surgery for an infiltrative basal cell carcinoma involving the perialar region (see image). What type of closure was performed?
-
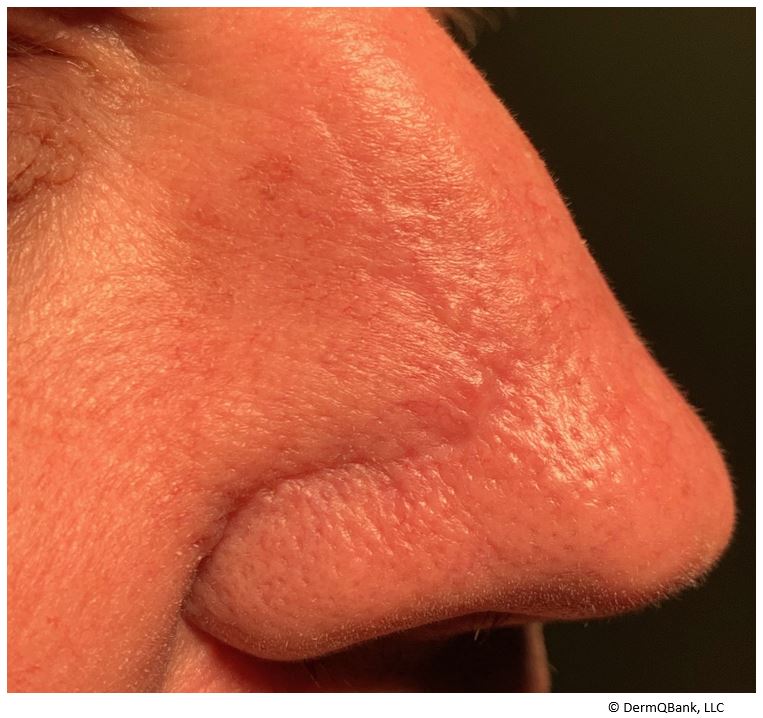
This is a crescentic advancement flap (a Burrow's triangle single tangent advancement flap).
Burrow’s Triangle Displacement Flaps (Tissue advancement, requires extensive undermining, depends on skin laxity and tissue elasticity)
- Burrow’s flap (Single tangent advancement flap)
- O to T flap (Bilateral single tangent advancement flap)
- A to T flap (Bilateral single tangent advancement flap)
- U flap (Double tangent advancement flap)
- H flap (Bilateral double tangent advancement flap)
- Curvilinear tangent advancement flap (Rotation, Karapandzic, Mustarde)
Defect Reconfiguration Flaps (Island pedicle flaps, tissue advancement depends on pedicle movement, blood supply from pedicle)
- Island pedicle flap (Kite flap, myocutaneous pedicle flap)
Tissue Reorientation Flaps (Reorientation of adjacent skin in area of laxity)
- Rhombic transposition flap (Limberg, Dufourmentel, Webster’s)
- Bi-lobed transposition flap
- Nasolabial transposition flap (Melolabial fold flap)
- Spear’s flap
Tissue Importation Flaps (Covering large wounds, cover avascular defects, two stages)
- Paramedian forehead flap (Indian flap)
- Nasolabial interpolation flap
- Retroauricular pedicle flap (Pin back flap)
- Modified Hughes flap
- Abbe cross-lip flap
Advancement Flaps (Utilize laxity adjacent to the wound. Incision made on either side of wound and tissue moved linearly)
- O to T advancement flap
- A to T advancement flap
- Island pedicle advancement flap
- Post auricular advancement flap
Rotation Flaps (Utilize tissue at a distant site, which is then rotated and draped over the wound)
- O to Z
- Mustarde rotation flap
- Back cut rotation flap
- Spiral rotation flap
- Dorsal nasal flap
- Glabella turndown flap
Transposition Flaps (Move donor tissue over normal tissue to the site of the defect. All transposition flaps create a secondary defect which requires closure)
- Z-plasty transposition flap
- Rhombic transposition flap
- Paramedian forehead transposition flap
- Bi-lobed transposition flap
- Flag transposition flap
- Banner transposition flap
Interpolation Flaps (Two-stage flaps in which the base of the flap is not immediately adjacent to the recipient site. They can tunnel under or bridge over normal skin)
- Axial interpolation flap
- Island pedicle flap
Clinical Pearl: A simplified way of looking at flaps is to divide them into advancement, rotation, transposition, and interpolation flaps.
- Advancement flaps: Utilize laxity adjacent to the wound, an incision is made on either side of the wound, and tissue is moved in a linear fashion to cover the defect
- Rotation flaps: Utilize tissue at a distant site, which is then rotated and draped over the wound
- Transposition flaps: Move donor tissue over normal tissue to the site of the defect. All transposition flaps create a secondary defect which requires closure
- Interpolation flaps: Two-stage flaps in which the base of the flap is not immediately adjacent to the recipient site. They can tunnel under or bridge over normal skin.