The picture demonstrates a typical dermoscopic appearance of which of the following lesions?
Benign and Malignant Neoplasms of the Skin
U
C
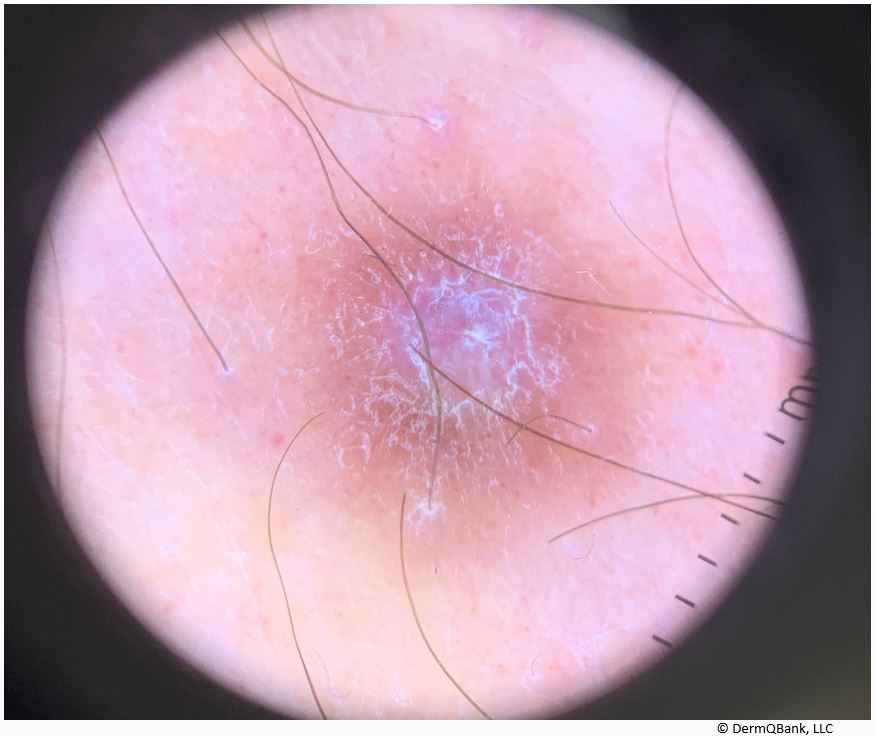
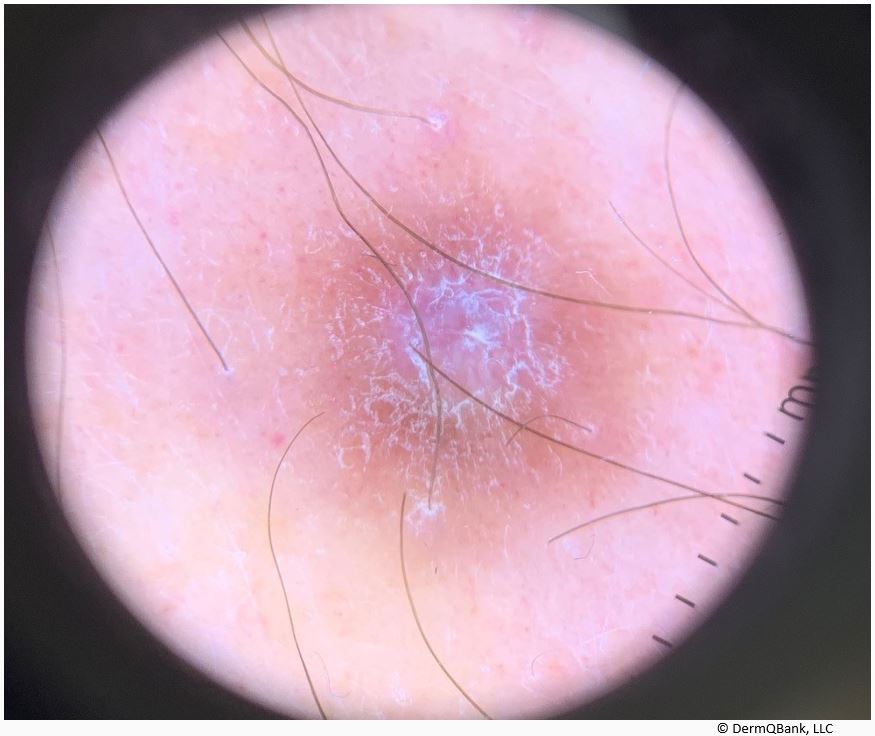
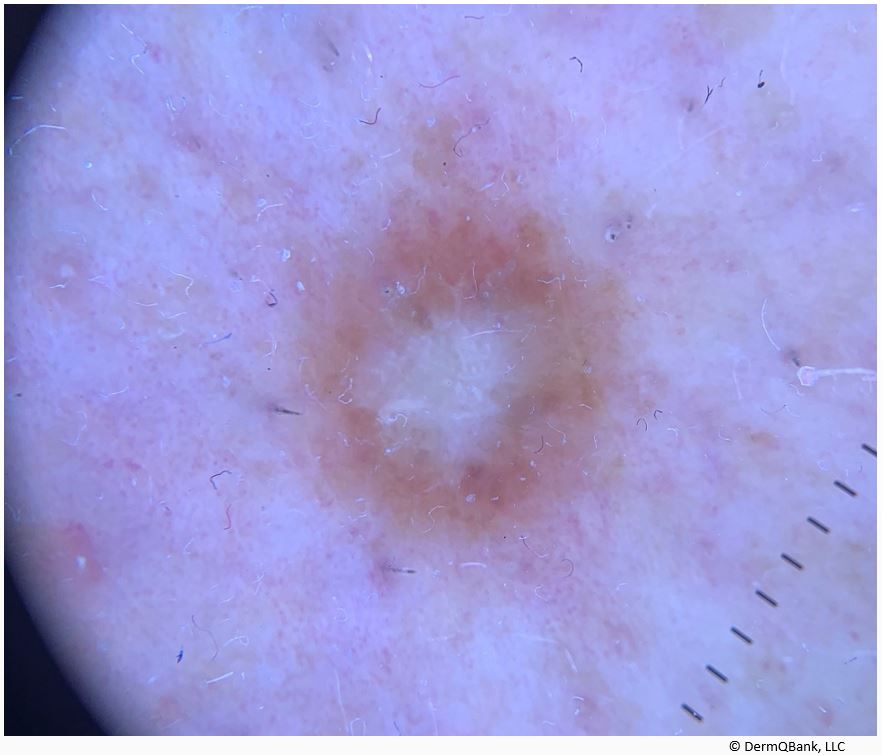
This is a classic dermoscopic appearance of a benign dermatofibroma (DF); a central white area similar to a scar surrounded by a discrete pigment network.
The white patchy area located centrally represents a clear (Grenz) zone from the spindle cell tumor (fibroblast-like spindle cells and histiocytes) in the dermis.
The confluent peripheral pigment represents hyperplastic epidermis (induction), elongated rete, and basal layer hyperpigmentation. (Puig et al. Arch Dermatol 2005)
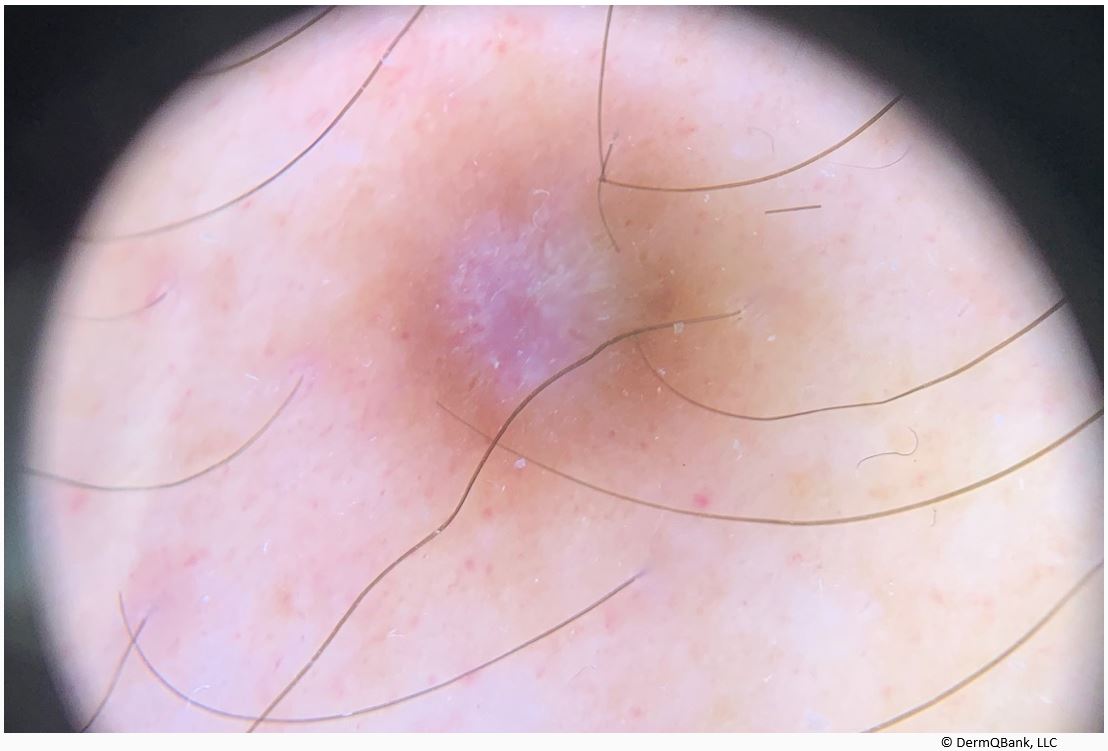
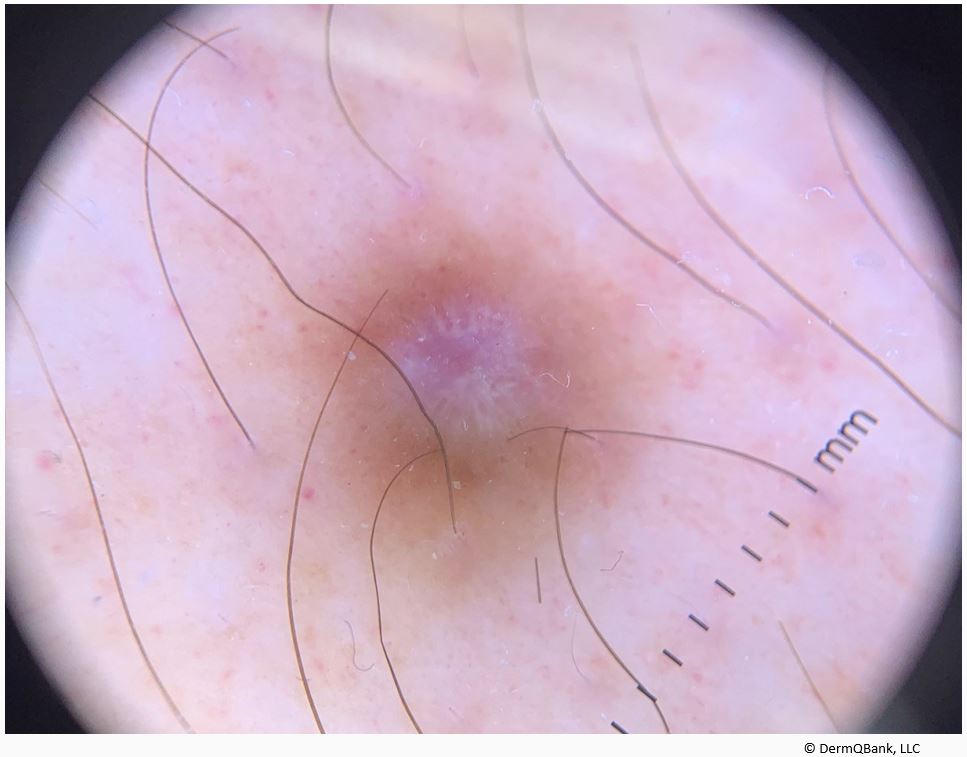
The dermoscopic features of a DF may differ based on anatomic site and variability does occur. A review of the dermoscopic variability of DF can be found in the following article (Espasandin-Arias et al. J Am Acad Dermatol 2015). Of note, dermoscopy of these lesions can deviate from the classic appearance and may mimic both benign and malignant skin tumors.
Clinical Pearl: Dermatofibromas are common benign tumors composed of fibroblast-like spindle cells, histiocytes, and varying proportions of capillaries/vessels. Although the dermoscopic findings of dermatofibromas can vary, the classic dermoscopic appearance of a dermatofibroma is a central white area surrounded by a discrete pigment network. See images below.
Heads up! You can use keyboard for test navigation: press → for Next,
← for Previous, M for Mark/Unmark, P for Pause,
R for Review, A,B,C,... or 1,2,3,... to select answer.